

*UP, LA contributed equally
Introduction
A significant proportion of lower risk (LR)-MDS patients present with thrombocytopenia, being associated with shortened survival and higher risk of progression to acute myeloid leukemia (AML). Treatment options for patients with LR-MDS and severe thrombocytopenia remain limited apart from transfusion support. Romiplostim (ROM), a thrombopoietin receptor agonist (TPO-RA) has shown safety and efficacy dependent on endogenous TPO levels as well as platelet transfusion history in a poorly defined subset of LR-MDS patients (Giagounidis et al. Cancer 2014, Sekeres et al. BJH 2014).
Methods
The multicenter phase 2 EUROPE trial investigated potential biomarkers of response (e.g. TPO levels, molecular markers) to single agent ROM in LR-MDS patients with severe thrombocytopenia. Patients were eligible if platelet counts were ≤30 G/L or ≤50 G/L in case of bleeding history. The primary efficacy endpoint was the rate of hematologic improvement of platelets (HI-P, according to IWG 2006 criteria) lasting for at least 8 weeks after 16 weeks of ROM (750µg SC qw) treatment. At the time of screening, patients were assigned into 3 different cohorts based on their previous platelet transfusion events (PTE) as well as centrally assessed TPO serum levels (A: TPO<500 ng/l, PTE<6 units/past year; B: TPO<500 ng/l, PTE≥6 units or TPO≥500 ng/l, PTE<6 units, C: TPO≥ 500 ng/l, PTE≥6 units). Bone marrows analysis were centrally reviewed.
Results
From 2015 to 2019, a total of 79 patients were included at 29 trial sites in Germany, France and the Czech Republic. Patients' median age was 74 years (range 42-93), median baseline platelet count was 25.5 G/L (range 3-50 G/L) and they were stratified into cohort A (n=51) or B+C (n=28), respectively. The primary endpoint was met with 34 out of 79 (43%) patients responding (HI-P), with response being markedly higher in cohort A (49%, n=25) vs. cohort B and C (32%, n=9) (p=0.145). Ten (13%) and eight (10%) patients had additional neutrophil (HI-N) and erythroid (HI-E) responses, respectively. During treatment, six patients had transient increases in peripheral blasts to more than 10% and one patient progressed to AML after one month of ROM. Although a higher number of responders was observed in group A, neither TPO level at screening (p=0.21), nor number of pretreatment PTE (p=0.12) were significantly associated with response to ROM treatment. Thus, our findings do not confirm that baseline TPO levels and number of pretreatment PTE alone allow reliable prediction of response to ROM.
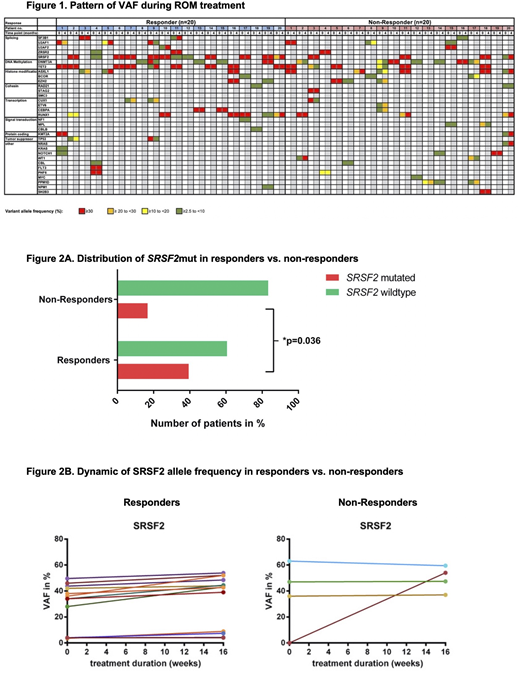
With the aim to identify new molecular patterns correlating with response, we performed a targeted NGS analysis for somatic variants in 54 candidate genes in 75 patients at baseline and in 44 patients after 16 weeks of ROM. Responders (R) more frequently exhibited mutations like SRSF2 (R=39%, NR=17%), RUNX1 (R=24%, NR=14%) and TET2 (R=30%, NR=29%), whereas non-responders (NR) exhibited mutations like DNMT3A (R=12%, NR=21%), U2AF1(R=9%, NR=14%) or ASXL1 (R=6%, NR 17%) more frequent. The percentages of patients with a response to ROM were similar regardless of total number of baseline somatic mutations. Comparing responders vs. non-responders, we found no significant changes of variant allelic burden of variants detected pre- and post-ROM (Fig. 1).
We identified the presence of a SRSF2 mutation as a significant predictor of response to ROM treatment (p=0.031, logistic regression). Mutated SRSF2 was significantly more frequent in responders (39%) compared to non-responders (17%) (p=0.036, Fisher's exact test) (Fig. 2A,B). We used logistic regression with stepwise backward selection to assess the influence of the presence of ASXL1, DNMT3A, RUNX1, TET2 and SRSF2 mutations on response. Our final regression model excludes the non-significant ASXL1, DNMT3A, RUNX1 and TET2 mutations and includes the significant SRSF2 mutation, resulting in an overall accuracy of 64.0% for a correct ROM response prediction in this patient cohort.
Conclusion:
This prospective study did not confirm a significant association between response to ROM, pretreatment PTE burden and endogenous TPO levels. Instead, patients with a mutated SRSF2 displayed a significantly higher response to ROM treatment. This may allow personalized treatment approaches in patients with LR-MDS and severe thrombocytopenia. In this study, extended treatment with ROM did not lead to a significant increase in AML cases.
Kubasch:Shire: Research Funding; Celgene: Research Funding; Novartis: Research Funding. Giagounidis:AMGEN: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Götze:Celgene: Research Funding. Cony-Makhoul:Novartis: Consultancy; Pfizer: Consultancy; Incyte Biosciences: Speakers Bureau; BMS: Consultancy; BMS: Speakers Bureau. Laribi:takeda: Research Funding; novartis: Honoraria, Research Funding; amgen: Research Funding; abbvie: Honoraria, Research Funding. Park:Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Other: Travel expenses. Metzeler:Astellas: Honoraria; Otsuka Pharma: Consultancy; Pfizer: Consultancy; Jazz Pharmaceuticals: Consultancy; Novartis: Consultancy; Celgene: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Honoraria. Thiede:AgenDix GmbH: Other: Co-owner and CEO. Schlenk:PharmaMar: Research Funding; Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees, Other: Travel, Accomodations, Expenses, Research Funding, Speakers Bureau; Novartis: Speakers Bureau; Roche: Research Funding; AstraZeneca: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Fenaux:Novartis: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding; Jazz: Honoraria, Research Funding; BMS: Honoraria, Research Funding. Platzbecker:Novartis: Consultancy, Honoraria, Research Funding; Amgen: Honoraria, Research Funding; BMS: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; Geron: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Research Funding. Ades:Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Research Funding; takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; novartis: Research Funding; Celgene/BMS: Research Funding; jazz: Membership on an entity's Board of Directors or advisory committees, Research Funding.
Romiplostim is a thrombopoietin receptor agonist indicated for the treatment of thrombocytopenia in patients with chronic immune thrombocytopenia (ITP). Limitations of Use: Romiplostim is not indicated for the treatment of thrombocytopenia due to myelodysplastic syndrome (MDS) or any cause of thrombocytopenia other than chronic ITP.

